Treatment Approach for Advanced Gastrointestinal Stromal Tumor (GIST): Safety and Efficacy Data
Important Safety Information
There are no contraindications for QINLOCK.
Palmar-plantar erythrodysesthesia syndrome (PPES): In INVICTUS, Grade 1-2 PPES occurred in 21% of the 85 patients who received QINLOCK. PPES led to dose discontinuation in 1.2% of patients, dose interruption in 2.4% of patients, and dose reduction in 1.2% of patients. Based on severity, withhold QINLOCK and then resume at same or reduced dose.
New Primary Cutaneous Malignancies. In INVICTUS, cutaneous squamous cell carcinoma(cuSCC) occurred in 4.7% of the 85 patients who received QINLOCK with a median time to event of 4.6 months (range 3.8 to 6 months). In the pooled safety population, cuSCC and keratoacanthoma occurred in 7% and 1.9% of patients, respectively. In INVICTUS, melanomaoccurred in 2.4% of the 85 patients who received QINLOCK. In the pooled safety population, melanoma occurred in 0.9% of patients. Perform dermatologic evaluations when initiating QINLOCK and routinely during treatment. Manage suspicious skin lesions with excision and dermatopathologic evaluation. Continue QINLOCK at the same dose.
Hypertension: In INVICTUS, Grade 1-3 hypertension occurred in 14% of the 85 patients who received QINLOCK, including Grade 3 hypertension in 7% of patients. Do not initiate QINLOCK in patients with uncontrolled hypertension. Monitor blood pressure as clinically indicated. Based on severity, withhold QINLOCK and then resume at same or reduced dose or permanently discontinue.
Cardiac Dysfunction: In INVICTUS, cardiac failure occurred in 1.2% of the 85 patients who received QINLOCK. In the pooled safety population, cardiac dysfunction (including cardiac failure, acute left ventricular failure, diastolic dysfunction, and ventricular hypertrophy) occurred in 1.7% of patients, including Grade 3 adverse reactions in 1.1% of patients.
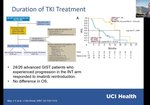
In INVICTUS, Grade 3 decreased ejection fraction occurred in 2.6% of the 77 patients who received QINLOCK and who had a baseline and at least one post-baseline echocardiogram. Grade 3 decreased ejection fraction occurred in 3.4% of the 263 patients who received QINLOCK and who had a baseline and at least one post-baseline echocardiogram.
In INVICTUS, cardiac dysfunction led to dose discontinuation in 1.2% of the 85 patients who received QINLOCK. The safety of QINLOCK has not been assessed in patients with a baseline ejection fraction below 50%. Assess ejection fraction by echocardiogram or MUGA scan prior to initiating QINLOCK and during treatment, as clinically indicated. Permanently discontinue QINLOCK for Grade 3 or 4 left ventricular systolic dysfunction.
Risk of Impaired Wound Healing: QINLOCK has the potential to adversely affect wound healing. Withhold QINLOCK for at least 1 week prior to elective surgery. Do not administer for at least 2 weeks following major surgery and until adequate wound healing. The safety of resumption of QINLOCK after resolution of wound healing complications has not been established.
Photosensitivity: QINLOCK may cause photosensitivity reactions. In 621 patients treated with QINLOCK in clinical trials, photosensitivity reactions occurred in 0.6% of patients. Advise patients to limit direct ultraviolet exposure during treatment with QINLOCK and for at least 1 week after discontinuation of treatment.
Embryo-Fetal Toxicity: QINLOCK can cause fetal harm when administered to a pregnant woman. Advise pregnant women of the potential risk to a fetus. Advise females of reproductive potential and males with female partners of reproductive potential to use effective contraception during treatment and for 1 week after the last dose. Because of the potential for serious adverse reactions in the breastfed child, advise women not to breastfeed during treatment and for 1 week after the last dose. QINLOCK may impair fertility in males of reproductive potential.
Adverse Reactions: The most common adverse reactions (≥20%) were alopecia, fatigue, nausea, abdominal pain, constipation, myalgia, diarrhea, decreased appetite, PPES, and vomiting. The most common Grade 3 or 4 laboratory abnormalities (≥4%) were increased lipase and decreased phosphate.
The safety and effectiveness in pediatric patients have not been established.
Administer strong CYP3A inhibitors with caution. Monitor patients who are administered strong CYP3A inhibitors more frequently for adverse reactions. Avoid concomitant use with strong and moderate CYP3A inducers. If a moderate CYP3A inducer cannot be avoided, increase QINLOCK dosing frequency from the recommended dose of 150 mg once daily to 150 mg twice daily during the co-administration period. If the concomitant moderate CYP3A inducer is discontinued, resume QINLOCK dosage back to 150 mg once daily 14 day after the discontinuation of the moderate CYP3A inducer.
Please see Prescribing Information, including Patient Information.
To report SUSPECTED ADVERSE REACTIONS, contact Deciphera Pharmaceuticals, LLC, at 1-888-724-3274 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DCPH-P01606